
Abstract
Carfilzomib, a second-generation proteasome inhibitor, has emerged as a cornerstone in the treatment of relapsed and refractory multiple myeloma (R/RMM). Building on the limitations of first-generation inhibitors like Bortezomib, Carfilzomib offers enhanced specificity, reduced toxicity, and improved patient outcomes. This blog delves into the biochemical mechanisms that underpin Carfilzomib’s therapeutic efficacy, including its irreversible inhibition of proteasomal activity and modulation of apoptotic pathways. Key clinical trials are reviewed, highlighting Carfilzomib’s significant impact on overall response rates and survival metrics. Additionally, the post explores the future potential of Carfilzomib in combination therapies and its role in overcoming drug resistance. As research advances, Carfilzomib continues to shape the landscape of multiple myeloma treatment, offering hope for improved survival and quality of life for patients.
Keywords: Carfilzomib, Multiple Myeloma, Proteasome Inhibitor, Relapsed/Refractory Cancer, Apoptosis Mechanism
Introduction to Multiple Myeloma and the Role of Proteasome Inhibition
MM is a prevalent hematologic malignancy, and it can turn out to be extremely harmful. In the United States, it is estimated that 24,050 new cases of MM (13,500 in men and 10,550 in women) will be diagnosed during 2014 with an expected death rate among affected individuals up to as high as approximately as high nearly. During the past few years, advancements in new and better drugs for treating MM have been made. Already in clinical trials as monotherapy and combination with older agents, these drugs have contributed to a plethora of next-generation therapeutic options for MM patients in short order leading to survival benefit not only response rate (RR) but rather overall-survival(OS). Bortezomib, carfilzomib (second-generation PIs), pegylated liposomal doxorubicin and the immunomodulatory compounds thalidomide, lenalido
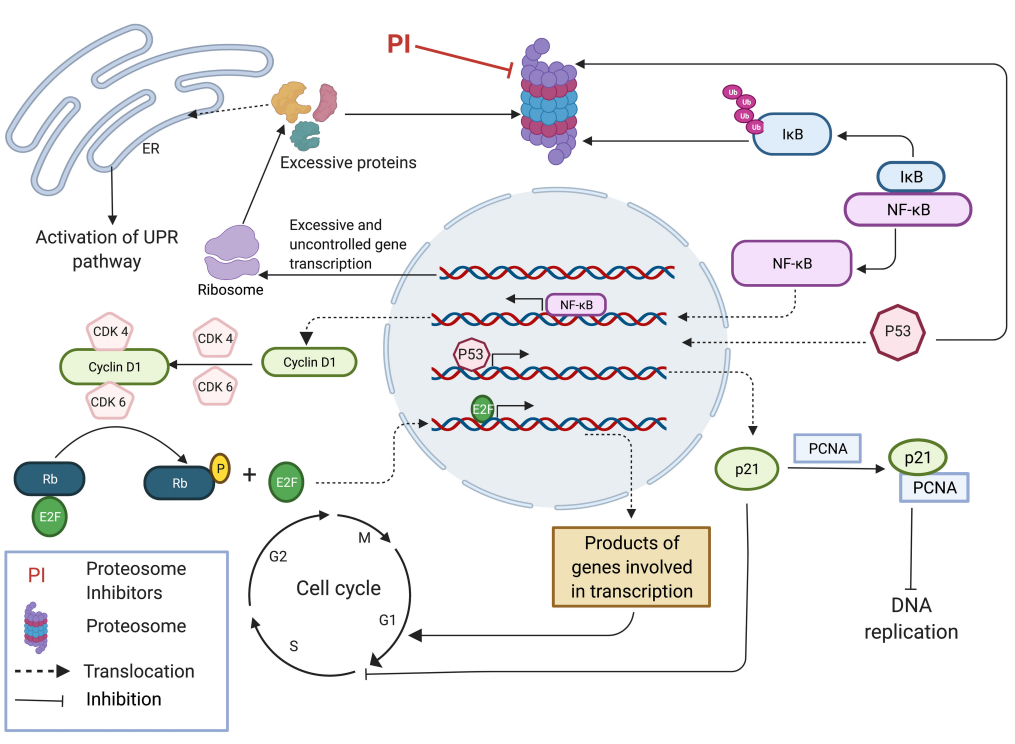
The 20S proteasome, the catalytic core of these complexes and responsible for protein degradation is targeted with the PIs leading to their antineoplastic activity. The proteasome catalytic core consists of chymotrypsin-, trypsin- and caspase-like proteolytic activities, thereby channeling proteins for degradation in a ubiquitin-independent manner. The rate-limiting step in the proteolytic process is due to intrinsically low chymotrypsin-like activity, and its inhibition compromises cell survival. Proteasome inhibition consequences are the followings: i) accumulation of misfolded proteins that activates endoplasmic reticulum stress, unfolded protein response (UPR), and apoptosis; ii) induction of autophagy; iii) inhibition on the nuclear factor-kB pathway, which regulates cell proliferation and survival due to blockade in IkB degradation-pathway inhibitor for this activity as well as iv); stabilization pro-apoptotic proteins/tumor suppressor gene products also deregulation cyclins/cyclin kinases /cycklin inhibitors. Large amounts of misfolded or unfolded immunoglobulins are produced by malignant plasma cells, and to rid themselves of these abnormal proteins they depend on their protein handling machinery including the proteasomer. There is an extensive literature of overexpression of the idiopathic subunits and components responsible for unfolded protein response (UPR) in hematological malignancies. This makes malignant plasma cells specifically sensitive to proteasome inhibition. The first proteasome inhibitor approved by the FDA for treatment of newly diagnosed MM (NDMM) as well as relapsed/refractory MMC(RR-MM). It is a reversible dipeptide boronate that targets the chymotrypsin-like (beta 5) and, to some extent, the caspase-like (beta 1), activities of the proteasome. However, resistance to bortezomib or the development of treatment-induced peripheral neuropathy (PN) often beings about drug discontinuation and limits therapeutic duration in patients. Despite ISP-34, the rate of bortezomib-induced PN is somewhat decreased with SC route of administration (38%), from which remains substantial.
In 2012, the US FDA approved carfilzomib in patients with MM who received ≥ two lines of therapies inclusive bortezomib and an IMiD; progression on or within 60 days from completion of last therapy.
Mechanistic Insights: How Carfilzomib Induces Tumor Cell Death
Carfilzomib exerts its anti-tumor effects primarily through the irreversible inhibition of the proteasome, a critical enzyme complex responsible for degrading intracellular proteins. This inhibition disrupts the ubiquitin-proteasome pathway, leading to the accumulation of misfolded and damaged proteins within the cell. The resulting endoplasmic reticulum (ER) stress triggers the unfolded protein response (UPR), which can induce apoptosis if the stress is severe and prolonged. Additionally, Carfilzomib stabilizes the tumor suppressor protein p53, enhancing its pro-apoptotic functions and leading to cell cycle arrest and programmed cell death.
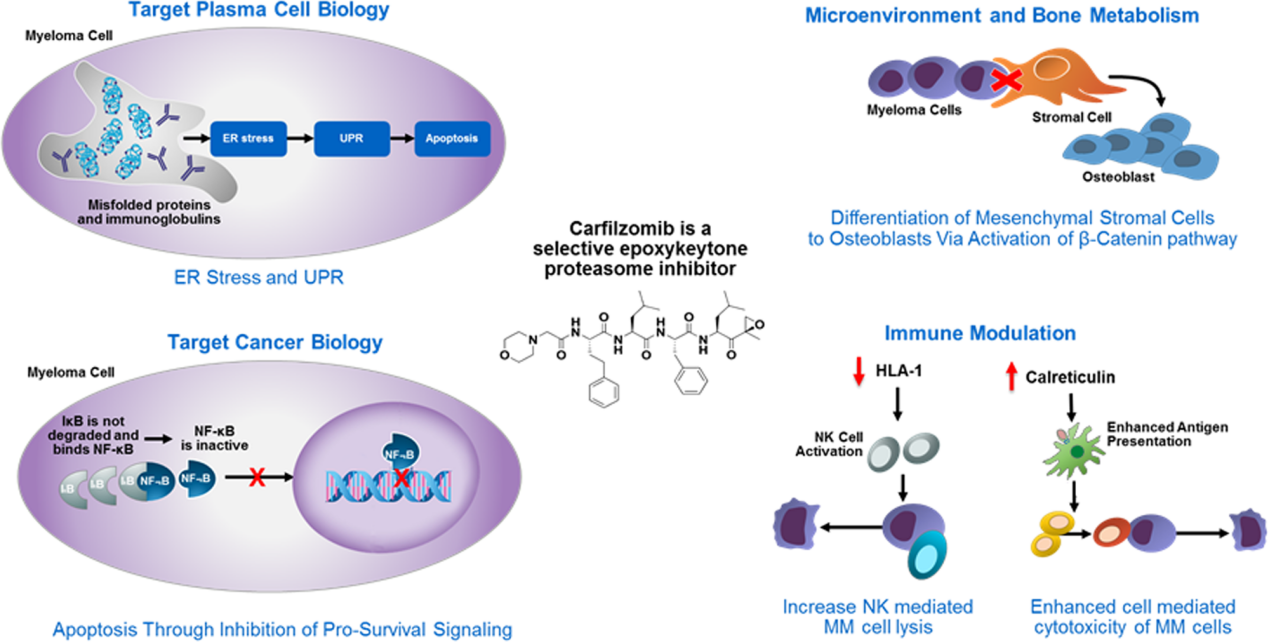
The specificity of Carfilzomib for the β5 subunit of the 20S proteasome and its immunoproteasome counterpart, LMP7, ensures that the drug effectively targets cancer cells while minimizing damage to normal cells. This selective inhibition is crucial, as it leads to the disruption of critical survival pathways in multiple myeloma cells, including the nuclear factor-kappa B (NF-κB) pathway. The inhibition of NF-κB, a key regulator of cell proliferation and survival, further enhances the pro-apoptotic effects of Carfilzomib.
Clinical studies have demonstrated that Carfilzomib induces apoptosis through both intrinsic and extrinsic pathways, involving caspase-3, -8, and -9 activation. Moreover, Carfilzomib’s rapid clearance from the bloodstream reduces the risk of off-target effects, making it a highly potent and tolerable option for patients with relapsed and refractory multiple myeloma. This mechanism of action not only underpins Carfilzomib’s efficacy but also its ability to overcome resistance seen with earlier proteasome inhibitors.
Clinical Efficacy of Carfilzomib in Treating Relapsed/Refractory Multiple Myeloma
Carfilzomib has been rigorously evaluated in numerous clinical trials, establishing its efficacy in patients with relapsed and refractory multiple myeloma (R/RMM). One of the pivotal studies, the PX-171-003-A1 trial, demonstrated that Carfilzomib monotherapy produced an overall response rate (ORR) of 23.7% in heavily pretreated patients, with a median progression-free survival (PFS) of 3.7 months and an overall survival (OS) of 15.6 months. These results were significant given the limited treatment options for this patient population.
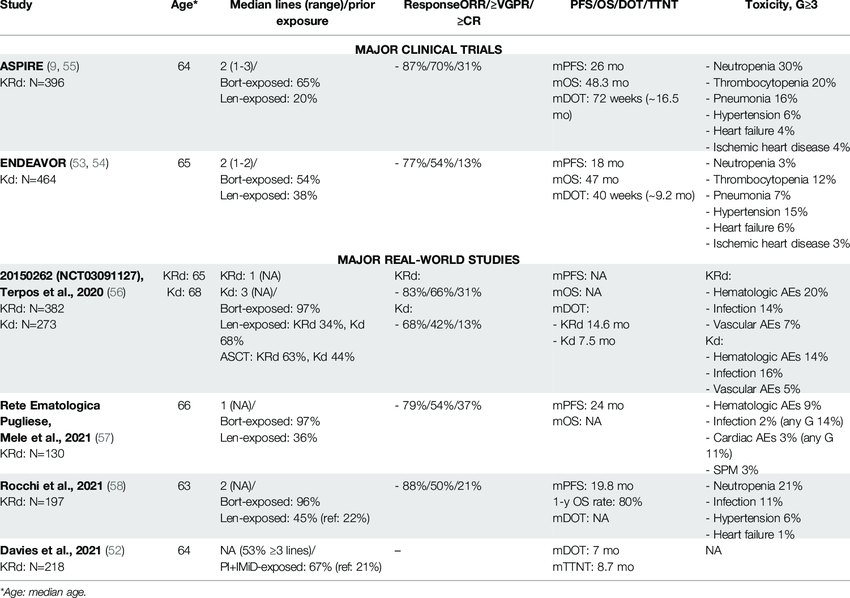
The ENDEAVOR trial further solidified Carfilzomib’s role in combination therapy. In this Phase III study, Carfilzomib combined with dexamethasone (Kd) was compared to Bortezomib with dexamethasone (Vd). The results showed a significant improvement in median PFS (18.7 vs. 9.4 months) and ORR (77% vs. 63%) in favor of the Kd regimen. Additionally, the median OS was extended by 7.6 months in the Carfilzomib group.
The ASPIRE trial evaluated Carfilzomib in combination with lenalidomide and dexamethasone (KRd) versus lenalidomide and dexamethasone alone (Rd). This trial reported an impressive median PFS of 26.3 months for the KRd group compared to 17.6 months for the Rd group. The ORR was also higher in the KRd group (87.1% vs. 66.7%). These results led to the widespread adoption of Carfilzomib as part of combination regimens for treating R/RMM.
These trials underscore Carfilzomib’s effectiveness in extending survival and improving response rates in patients with R/RMM, making it a cornerstone in the management of this challenging disease.
Future Prospects: Enhancing Carfilzomib’s Therapeutic Potential
As Carfilzomib continues to demonstrate efficacy in the treatment of relapsed and refractory multiple myeloma (R/RMM), future research is focused on optimizing its use and expanding its therapeutic potential. One key area of investigation is the development of combination therapies that include Carfilzomib with novel agents such as monoclonal antibodies, immunomodulatory drugs, and next-generation proteasome inhibitors. These combinations aim to enhance therapeutic outcomes, overcome resistance, and reduce toxicity.
Another significant challenge is addressing the mechanisms of resistance that some patients develop to Carfilzomib. Research is ongoing to understand these resistance pathways better and to identify biomarkers that can predict response to Carfilzomib-based therapies. Additionally, there is interest in exploring the use of Carfilzomib in solid tumors, given its potent anti-proteasome activity and ability to induce apoptosis in various cancer cell types.
Efforts are also being made to refine dosing regimens and administration schedules to improve patient convenience and minimize side effects. These advancements, coupled with continued clinical trials, are likely to expand the role of Carfilzomib in cancer therapy, making it a more versatile and effective treatment option for various malignancies.