
Abstract
Bremelanotide, a melanocortin receptor agonist, represents a significant advancement in the treatment of Hypoactive Sexual Desire Disorder (HSDD), a prevalent and challenging aspect of Female Sexual Dysfunction (FSD). By targeting the melanocortin-4 receptor, Bremelanotide effectively modulates neural pathways associated with sexual desire, distinguishing it from other treatments. This review provides an in-depth analysis of Bremelanotide’s mechanism of action, pharmacodynamics, and pharmacokinetics, alongside a detailed examination of clinical trial outcomes, particularly the Phase 3 RECONNECT studies. The safety profile and tolerability of Bremelanotide are also explored, emphasizing its efficacy across various patient subgroups. As ongoing research continues to expand its potential applications, Bremelanotide holds promise as a cornerstone in the therapeutic landscape for FSD. This article aims to contribute to the academic discourse on Bremelanotide by highlighting its clinical significance and future potential in addressing sexual dysfunction in women.
Keywords: Bremelanotide, Female Sexual Dysfunction (FSD), Hypoactive Sexual Desire Disorder (HSDD), Melanocortin Receptor Agonist, Clinical Trials
Introduction
Hypoactive sexual desire disorder (HSDD) is the most prevalent female sexual health disorder. HSDD is defined as persistent deficiency or absence of sexual fantasies and desire, resulting in significant distress or interpersonal difficulty. The criteria based on the Diagnostic and Statistical manual are “persistently or recurrently deficient (or absent) sexual fantasies and desire for sexual activity: that causes marked distress or interpersonal difficulty”. Women with this disorder may display a lack of motivation for sexual activity, reduced responsiveness to erotic cues, a loss of interest during sexual activity, and avoidance of situations that could lead to sexual activity. Women who suffer from HSDD commonly have reduced self-confidence, self-worth, and impaired body image. Diagnosis of HSDD requires personal distress and a change in sexual desire for a least three months. Subtypes of HSDD include those that are due solely to “psychological factors” and “combined factors.” The HSDD can be due to psychological factors, substances, or medical conditions in the combined subtype. The overall prevalence of HSDD ranges from 8–19%. The prevalence of HSDD increases with age and has a higher prevalence in postmenopausal women. The risk is the greatest in younger women in surgical menopause and is associated with a less active sex life and decreased sexual and relationship satisfaction. Women who are premenopausal and experience hypoactive sexual desire have higher levels of distress than postmenopausal women and are more likely to seek help. Women with distressing low sexual desire have a poorer health-related quality of life. Women suffering from this disorder have reported decreased physical functioning, vitality, social functioning, general health, mental health, and a loss of femininity.
Several factors have been proposed to explain the etiology of low sexual desire and the accompanying distress. These factors include partners and life situation, ethnicity and culture, menopause status, central nervous system activity, and hormonal influences. Married women or women living with a spouse or partner were more likely to have distressing low sexual desire than single women. The PRESIDE study revealed that Caucasian women were more likely than Black women to have low sexual desire. Additionally, brain areas such as the cerebral cortex may play a role in women developing HSDD. When presented with erotic cues, women with HSDD were shown to have weaker cerebral cortex activation in the right hemisphere and less deactivation in the left hemisphere than women who did not have HSDD. Various drugs or conditions that decrease dopamine levels alter brain serotonin at serotonin 2A receptors or increase opioids at mu receptors have also been shown to reduce or inhibit sexual desire. Treatment of HSDD includes both psychosocial and biological therapies. Psychosocial therapies include cognitive behavioral therapy, sensate focus therapy, and mindfulness-based cognitive therapy. The current biological therapies for HSDD include flibanserin, testosterone therapy, bupropion (off-label treatment), and buspirone (off-label treatment).
Decoding the Mechanism: How Bremelanotide Modulates Sexual Desire
Bremelanotide is a groundbreaking therapeutic agent in the treatment of Hypoactive Sexual Desire Disorder (HSDD), operating through a novel mechanism as a melanocortin receptor agonist. Its primary action is centered on the melanocortin-4 receptor (MC4R), a crucial receptor in the central nervous system linked to sexual function. By binding to and activating MC4R, Bremelanotide effectively modulates neural pathways that influence sexual desire and arousal.
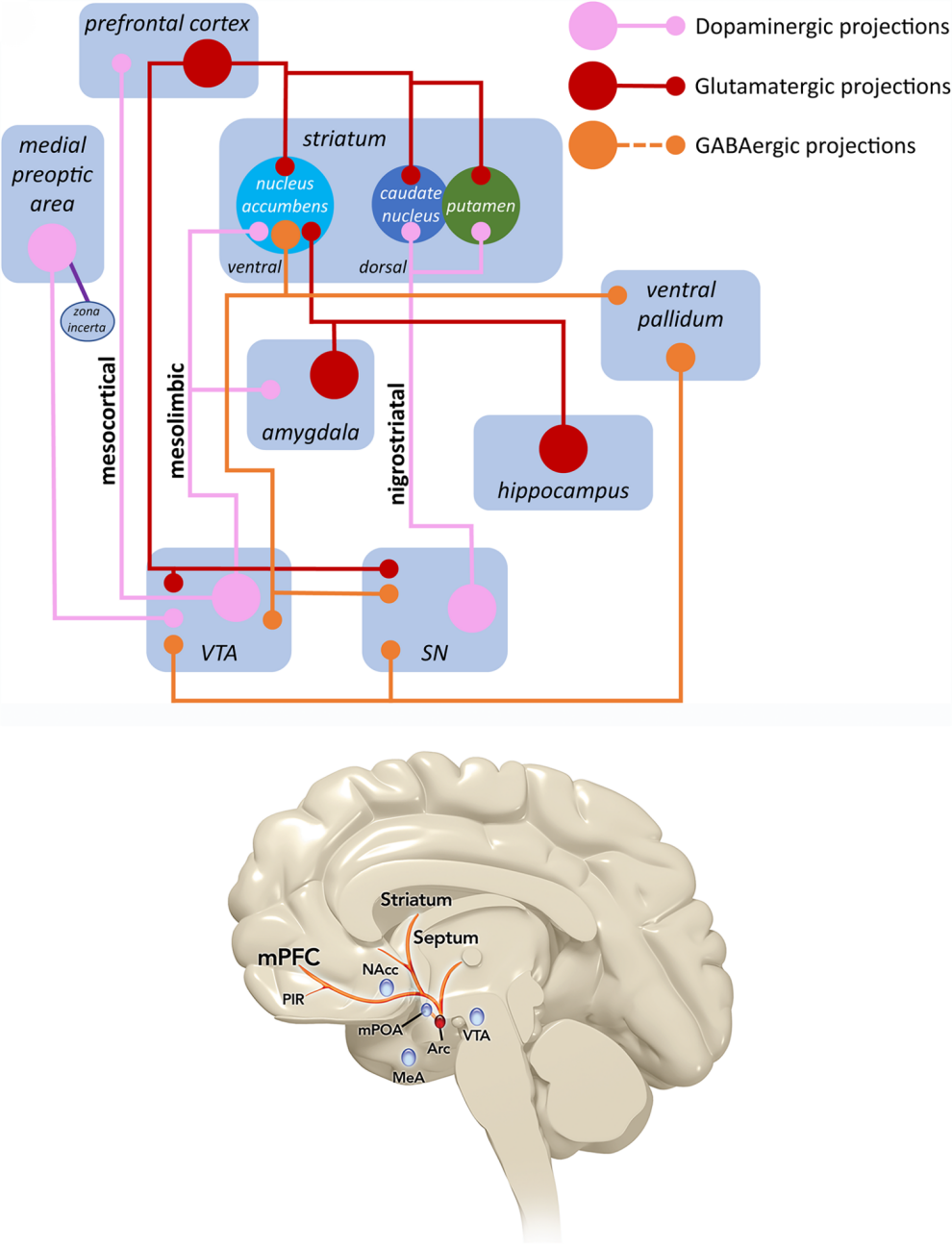
The pharmacodynamics of Bremelanotide involve its nonselective activation of several melanocortin receptor subtypes, including MC1R, MC3R, MC4R, MC5R, and MC2R, with a preference for MC4R and MC1R. The activation of MC4R in particular is associated with the regulation of sexual response, making it a pivotal target in the treatment of HSDD. This receptor’s role in enhancing sexual motivation and reducing sexual distress underscores Bremelanotide’s unique therapeutic profile.
Unlike other treatments for HSDD, such as flibanserin, which modulates serotonin levels, Bremelanotide directly influences the excitatory pathways involved in sexual desire. This direct action on the brain’s melanocortin system positions Bremelanotide as a potent and distinct alternative to existing therapies. The drug’s ability to be administered on demand further enhances its practicality and appeal, offering a flexible treatment option that aligns with individual patient needs.
Moreover, the safety profile of Bremelanotide is favorable, with clinical trials demonstrating minimal adverse effects, primarily mild and transient. The combination of its unique mechanism of action, efficacy in improving sexual desire, and favorable safety profile distinguishes Bremelanotide as a novel and promising treatment for women suffering from HSDD.
Efficacy and Outcomes: Clinical Trials Highlighting Bremelanotide’s Impact
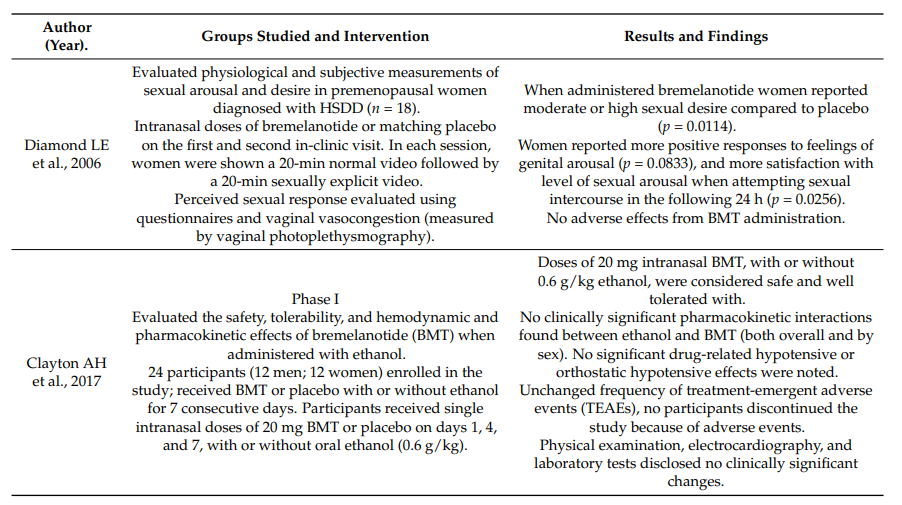
Bremelanotide has undergone rigorous clinical evaluation, particularly in its application for treating Hypoactive Sexual Desire Disorder (HSDD) in premenopausal women. The drug’s efficacy was most notably demonstrated in the Phase 3 RECONNECT studies, which were pivotal in securing its approval for clinical use.
The RECONNECT studies were large, randomized, double-blind, placebo-controlled trials that assessed the efficacy and safety of Bremelanotide in women diagnosed with acquired, generalized HSDD. The trials included over 1,200 premenopausal women who were in stable relationships and had experienced HSDD for at least six months. Participants were randomized to receive either Bremelanotide or a placebo, administered subcutaneously as needed, at a dose of 1.75 mg.
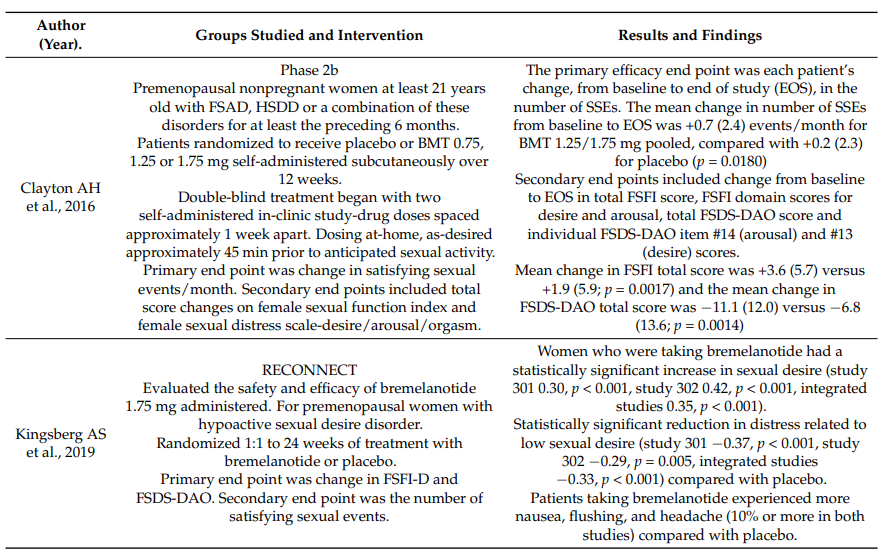
The primary endpoints of the RECONNECT studies were improvements in sexual desire and reductions in sexual distress. These were measured using validated tools such as the Female Sexual Function Index-Desire Domain (FSFI-D) and the Female Sexual Distress Scale-Desire/Arousal/Orgasm (FSDS-DAO). Bremelanotide showed statistically significant improvements in both primary endpoints compared to placebo. Specifically, there was a notable increase in the FSFI-D score and a significant decrease in the FSDS-DAO score, indicating enhanced sexual desire and reduced distress among the participants.
Secondary outcomes also favored Bremelanotide, including improvements in overall sexual satisfaction, orgasm, arousal, and lubrication. These findings were consistent across various subgroups, including different age groups and body weights, further supporting the drug’s broad applicability.
The extension phases of the RECONNECT studies, which spanned 52 weeks, confirmed the sustained efficacy of Bremelanotide, with participants continuing to report improvements in sexual function and overall satisfaction. These trials have established Bremelanotide as a robust and effective treatment option for women suffering from HSDD.
Assessing Safety: The Tolerability Profile of Bremelanotide
Bremelanotide has been extensively evaluated for its safety and tolerability in clinical trials, with data showing it to be generally well-tolerated among premenopausal women with Hypoactive Sexual Desire Disorder (HSDD). The Phase 3 RECONNECT studies, which were pivotal in its approval, provided comprehensive safety data that underscored its clinical viability.
The most common adverse events associated with Bremelanotide were mild to moderate in severity, with nausea, flushing, and injection-site reactions being the most frequently reported. Nausea, in particular, occurred in approximately 40% of patients, predominantly after the first dose, and was transient, typically resolving within two hours. Other less common adverse events included headache and vomiting, which led to treatment discontinuation in a small percentage of participants.
Importantly, the RECONNECT studies showed no significant long-term safety concerns. In the 52-week extension phase, where patients continued Bremelanotide use, the incidence of adverse events remained consistent with those observed during the core study phase. Notably, there were no reports of severe cardiovascular effects, which is significant given that other treatments for HSDD have been associated with such risks.
A key advantage of Bremelanotide over other treatments is its safety in conjunction with alcohol consumption. Unlike flibanserin, which carries a boxed warning for severe hypotension and syncope when used with alcohol, Bremelanotide does not exhibit such risks, making it a more flexible option for patients. Additionally, while Bremelanotide can cause transient increases in blood pressure and decreases in heart rate, these changes are typically mild and not clinically significant.
Overall, Bremelanotide’s safety profile is favorable, with a tolerability that supports its use as an on-demand treatment for HSDD. The lack of serious long-term adverse effects and the ability to use it alongside alcohol further enhance its appeal as a therapeutic option.
Exploring New Horizons: Future Directions for Bremelanotide in Sexual Dysfunction Treatment
Bremelanotide’s approval marked a significant milestone in the treatment of Hypoactive Sexual Desire Disorder (HSDD), yet its potential extends beyond current applications. Ongoing research is exploring new avenues for its use, particularly in expanding its therapeutic indications and optimizing its clinical utility.
One of the key areas of interest is the potential application of Bremelanotide in treating sexual dysfunction in postmenopausal women, a population that has received less attention in clinical trials. Preliminary studies suggest that the drug’s mechanism of action, through melanocortin receptor activation, could be beneficial in this demographic as well. Researchers are also investigating the efficacy of Bremelanotide in other forms of sexual dysfunction, such as Female Sexual Arousal Disorder (FSAD), where current treatment options are limited.
Another promising direction is the exploration of combination therapies involving Bremelanotide. By pairing it with other agents that target different aspects of sexual dysfunction, researchers hope to enhance its efficacy and broaden its therapeutic scope. For instance, combining Bremelanotide with selective serotonin reuptake inhibitors (SSRIs) could address both the psychological and physiological components of sexual dysfunction.
Furthermore, studies are underway to better understand the long-term effects of Bremelanotide use, particularly regarding its impact on cardiovascular health and its interactions with other medications. Given its favorable safety profile in short-term studies, long-term data could reinforce its role as a cornerstone treatment for HSDD and potentially other conditions.
Finally, the development of alternative formulations of Bremelanotide, such as oral or transdermal delivery systems, is being explored. These innovations could improve patient compliance and convenience, making the treatment more accessible to a broader population.
As research progresses, Bremelanotide is poised to play an increasingly important role in the management of sexual dysfunction, with the potential to significantly improve the quality of life for affected individuals.